Clinical Pearls: The environmental impact of inhalers
May 9, 2023
By: Layne Liberty
This article is part of a series appearing in Interactions
, our biweekly newsletter, written and researched by CSHP's students. We've created this series as a valuable learning activity for pharmacy students undertaking rotations at CSHP. Crafting these pieces not only helps students gain in-depth knowledge of specific conditions, treatments, and resources, it also helps them hone their skills in research, critical appraisal, evaluation, synthesis, and writing – all of which will serve them well in clinical practice. The Professional Practice Team works with the students to select hot topics that are of interest and utility to both the students and to you, the reader. We hope you enjoy this piece by one of our future colleagues! Let us know what you think: If you would like to provide any comments or constructive feedback for our students, please email us at [email protected].
Background
According to the 2018 report from the Canadian Chronic Disease Surveillance System, there are 3.8 million Canadians over the age of one living with asthma and two million living with chronic obstructive pulmonary disease (COPD).1 Both of these conditions are large burdens on the healthcare system due to medical costs and resource use. Additionally, asthma is more prevalent in younger working age groups, it has a major economic impact due to productivity loss2 The prevalence of these chronic conditions is expected to rise as the Canadian population ages and as air quality continues to deteriorate.3 Climate change is a defining challenge of the 21st century and one of the largest contributors to the emission of greenhouse gases (GHG) is the healthcare system.4 The Canadian healthcare sector is responsible for 4.6% of the total GHG emissions and over 200,000 tons of pollutants primarily coming from hospitals, pharmaceuticals and physician services.5 Climate change poses a great risk to respiratory disease because it causes increased concentrations of outdoor ozone (often seen as ‘smog’) and particulate matter at ground level.6 In addition, increased global temperatures cause increased amounts of pollen produced by each plant, as well as an earlier and longer pollen season and higher rates of mold proliferation.6 These environmental factors all aggravate respiratory disease leading to uncontrolled symptoms, inhaler overuse and higher risk of asthma and COPD exacerbations.7,8
The pressurized metered dose inhalers (pMDI) and breath actuated inhalers (BAI) contain hydrofluorocarbon (HFC) propellants. These propellants are used to atomize the medication containing droplets in order to deliver it to the patients respiratory system.9 These propellants are potent greenhouse gases (GHG) with high global warming potential (GWP), a metric used to examine a GHG ability to trap heat in the atmosphere compared to carbon dioxide (CO2), and depending on the type of HFC used, are 1400-3200 times more potent than CO2.9,10 The other inhaler devices such as dry powered inhalers (DPI) and soft mist inhalers (SMI) do not contain these propellants and therefore have a lower carbon footprint (CFP).10 The active primary ingredient(s) (API) in DPIs are dispersed into the respiratory system by the patient’s own inspiratory rate while the SMI device, also known as Respimat, utilizes a spring to create the force to drive the aqueous medication into the lungs.10
A CFP can be quantified and assessed by how much greenhouse gas (often described in CO2 equivalents (CO2eq)) is emitted during a product's life cycle (e.g., from manufacturing to distribution to use to destruction).12 A CO2eq is a unit used to allow direct comparison to CO2 by expressing the potential global warming effect of all GHG emissions relative to CO2.12 When selecting inhaler therapies, pharmacological factors such as the safety and efficacy of the medication and patient factors such as finger dexterity and inspiratory rate and volume are key factors; however, the environmental impacts of inhaler treatments are becoming an increasingly important consideration.10 Asthma and COPD carry a significant economic burden due to hospital admissions, physician visits and resource utilization.2 In addition, poor disease management, patient adherence issues, incorrect inhaler use, and misdiagnosis all contribute to increased healthcare spending and poor environmental outcomes.2,3,11,12 Applying the information presented in this article along with shared decision making with patients will help healthcare providers select a drug regimen that is environmentally conscious, safe and effective.
Role Of The Pharmacist
Pharmacists are leaders in healthcare and with Canada’s recently updated nationally determined contribution to reduce emissions by 40-45% below 2005 levels by 2030 and to reach net zero carbon emissions by 2050, its essential that pharmacist begin advocating and incorporating environmental sustainability into their practice.13 There is a growing number of resources and education available to aid healthcare providers in transitioning to prescribing and suggesting alternative low carbon inhalers, one being the primer and playbooks supplied by Creating A Sustainable Canadian Health System In A Climate Crisis (CASCADES). Pharmacists are in a unique position to educate prescribers, colleagues, and patients on environmentally sustainably practices including the proper use and disposal of inhalers, and alternative therapies available. Pharmacist led interventions in the hospital such as initiating smoking cessation, conducting medication reviews, inhaler technique training, and reviewing asthma and COPD action plans have all been proven to improve disease management, adherence, and quality of life outcomes.14,15,16 COPD and asthma are often primarily managed in the community; however, a patient admitted to the hospital presents an opportunity for the hospital pharmacist to make appropriate interventions.17Acute exacerbations of COPD, which are the main reason for unscheduled hospital admissions, exert a significant impact on patients’ quality of life as it accelerates disease progression and leads to increased mortality.17 Asthma exacerbations also have a negative impact on quality of life, as it contributes to lung function decline, systemic effects, and mortality.18 Pharmacists have the knowledge and ability to make interventions like education and training on inhaler technique and could take it one step further by implementing environmentally conscious practices like education on proper medication disposal, suggesting alternative low carbon inhalers and promoting de-prescribing where clinically appropriate.
Pharmacist led interventions to reduce the environmental impact of inhalers include the following:
Life Cycle Assessment of Inhalers and Ensuring Proper Disposal
Life cycle assessments have been completed on the different inhaler devices to determine the amount of GHG emitted during each phase from manufacturing to patient use to disposal. As mentioned, the GHGs emitted from the propellants in pMDIs are very potent, and from data presented in Table 1, an inhaler regimen for one patient over one year (3 salbutamol pMDIs and 12 Advair pMDIs) can be estimated to be the same as driving a gas car 1498km (that’s equivalent to a roadtrip from Banff, AB to Winnipeg, MB).19 The use and the disposal phase for a pMDI makes up approximately 85% of the total CFP, while the main contribution to the CFPs for the DPI/SMI inhalers are from the API and during the manufacturing stages of the life cycle20. If the manufacturing phases are the only contributing factor considered, then on average, the inhalers with the largest CFP are still pMDIs.20 In a study that compared the CFPs of tiotropium bromide (Spiriva®) Respimat® (both disposable and reusable devices) and ipratropium bromide (Atrovent®) pMDI, it was noted that ipratropium had a CFP that was 20 times greater than the disposable Respimat® device.21 The disposal phase of the Respimat® is the largest contributor to its CFP, so refill cartridges have been introduced to help mitigate the impact.22 The reusable Respimat® device can be refilled up to 6 times before the device needs to be replaced.22For example, if a patient is prescribed the Spiriva Respimat®, then this would translate into reducing the number of inhalers per year per patient from 12 to 2.
Improper pMDI disposal causes the residual propellants to be released into the atmosphere which increases its negative impact on the environment.
9 The most common disposal process for pMDIs is by incineration as the HFCs require thermal degradation to be destroyed.
10 When pMDIs are disposed of correctly, it translates to an estimated CO
2 emission savings of 3 to 17 kg per inhaler.
9 In Manitoba, British Columbia, Prince Edward Island and Ontario, there is a health product stewardship program that operates medication return programs through community pharmacies.
23 Hospital pharmacists, in provinces where this service is offered, can further their environmental advocacy by educating and providing resources for patients and other health care providers around proper medication recycling in their community. Pharmacists have a role in promoting environmental initiatives and can help push for changes in practice, therapeutic guidelines, and organizational policy (e.g. purchasing practices and formulary choice).
Ensuring Proper Inhaler TechniqueIncorrect inhaler technique reduces the delivery of medication into the patients' lungs which is associated with poor disease outcomes, increased hospital admissions, increased healthcare costs and medication waste, all contributing to a larger environmental impact.
15 Assessing a patient's appropriate inhaler technique allows pharmacists to assess therapeutic safety and efficacy and provides an opportunity to suggest environmentally conscious alternatives. Pharmacist led inhaler training has been proven to be effective with improvement in patient disease management and maintenance of proper technique.
24,25,26 Although study results on improper inhaler technique vary, a study conducted in Canada found that 59% of study participants made critical errors (removing cap/lid/opening mouthpiece before administration, shaking MDI before use and inhaling properly depending on type used), while using their inhalers.
27 Patients using pMDIs were also more likely to make critical errors in administration (93%) compared to patients using DPIs/SMIs (39%).
27 The main critical errors in pMDI use were the actuation of the device and proper inhalation, which are common mistakes as patients are consistently unable to coordinate these two steps.
27Assessing a patient's inspiration ability and hand dexterity are essential as a major component of a pMDIs CFP comes from the patient use phase. Incorrect pMDI inhaler technique not only leads to uncontrolled disease, it also causes an excess in propellant outflow and a higher requirement of reliever and maintenance canisters per year, both contributing to pMDIs environmental impact.
9 Utilizing a spacer device with a pMDI in patients that have difficulty inspiring at the correct speed and depth can help mitigate this issue by slowing down drug delivery and reducing medication waste.
9 Another issue with pMDI that affects patients and the environment, is the lack of a dose counter on the device. Without a dose counter, patients are more likely to throw away half full canisters or continue to use empty inhalers.
9 Many patients use methods to test for the presence of medication like spraying into the air to see if medication comes out, which is incorrect, as the spray may just be leftover propellant.
28 Education and counselling on proper dose counting methods such as keeping track of the doses administered for maintenance inhalers (dividing the total doses in the inhaler (found on the box) by the total number of doses per day), and reliever inhalers (write down the doses used after every administration) can help mitigate these issues.
28
Recommend Alternate Inhaler Therapies
The National Health Services (NHS) in the United Kingdom (UK) has done extensive research on the environmental impact of inhalers and is aiming to reduce the carbon impacts of inhalers by 50% by 2030.29 0The Canadian healthcare system and health care providers can learn from this plan and join the NHS in making strides towards reducing healthcare’s environmental impact. Metered dose inhalers comprise 75% of the total amount of inhalers prescribed in Canada and the United States.9 Reliever medications like salbutamol (short-acting beta-2 agonist (SABA)) and ipratropium (short-acting muscarinic-antagonist (SAMA)) come in pMDI canisters and are commonly prescribed due to their treatment versatility (e.g. used for symptom management caused by conditions other than asthma and COPD) and low cost. Reliever and maintenance therapy metered dose inhaler prescriptions account for approximately 0.03% of annual global GHG emissions.9 and the carbon footprint of two doses of a salbutamol pMDI has been estimated to be approximately 500 g CO2e.19 In comparison, the CO2e emissions of a nine-mile car trip (approximately 14km) is estimated to be 2610 g CO2eq (only 5 puffs of a salbutamol pMDI).19 When these values are scaled up to a population level, one can understand how patients with uncontrolled respiratory disease are significantly contributing to GHG emissions. Metered dose inhaler use is a double-edged sword, because although it helps patients maintain control of their respiratory symptoms and disease, it also contributes to deteriorating air quality. Poor air quality is known to be a significant trigger for patients with respiratory disease and leads to increased risk of exacerbations and poor symptom control. Recommending alternative therapies is not as simple as just switching to a more environmentally conscious choice, there are other considerations to keep in mind such as commercial availability, economic burden, drug coverage and patient preference (e.g. ease of use, hand dexterity and strength of lungs). DPI and SMI devices carry a significantly lower environmental burden so switching to these devices when clinically appropriate is recommended.19 For example, fluticasone propionate/salmeterol combination is available as a pMDI and a DPI, so depending on the patients’ dose, this switch could help lower the carbon footprint. Other examples of switching to low carbon inhaler alternatives are described in Figure 119 and the CFP of commonly prescribed inhalers is found in Figure 2.19,20
Ensure Proper Diagnosis And Promote De-prescribing Where Clinically Possible
COPD requires spirometry testing before definitive diagnosis with a post-bronchodilator forced expiratory volume in one second to forced vital capacity (FEV1/FVC) ratio < 70%.
30 Diagnosing COPD just based on symptoms contributes to unnecessary treatment, patient psychological stress and overprescribing of inhalers.
30 Asthma is diagnosed based on respiratory symptoms in addition to evidence of variable expiratory airflow limitation, tested by either peak flow or spirometry.
31 A Canadian study of 613 patients with an asthma diagnosis in the last 5 years were re-tested with home peak flow and symptom monitoring, spirometry, and serial bronchial challenge tests.
32 It was discovered that 33% of the participants did not have asthma and after 12 months of follow-up, 30% patients still showed no clinical or lab evidence of asthma.
32 Similarly, overdiagnosis of COPD is common and it has been estimated that 1 in every 3 patients do not have COPD.
33,34,35 A population-based cohort study found that of 1403 randomly selected patients from Ontario (taken from the Canadian Cohort Obstructive Lung Disease (CanCOLD) study) 5.1% of patients did not have COPD, while only 3.7% had correctly diagnosed COPD.
36 Additionally, the over diagnosed COPD patients had significantly higher rates of hospitalizations, emergency department visits and ambulatory care visits.
36 Another study in Ontario from 2000-2010 of 491,754 patients with newly diagnosed COPD found that only about one-third received spirometry prior to diagnosis.
37 The Canadian Thoracic Society emphasizes the importance of de-prescribing inhaler therapies if the patient has not had a clinical benefit or confirmation of reversible airflow limitation through spirometry or peak flow testing.
30The misdiagnosis and overprescribing of inhaler treatments increases risk for patient adverse effects and contributes to the use of healthcare resource and waste production. Focusing on more thorough diagnosis practices, gathering in-depth patient medical history and inquiring about inhaler effectiveness to the patient can all contribute to decreasing the CFP of the healthcare sector.
Summary
The prevalence of asthma and COPD is expected to increase as the population ages and people are exposed to more environmental pollutants due to climate change. Asthma and COPD carry a significant environmental burden due to pMDI use, misdiagnosis and incorrect inhaler use. The use and disposal phase for pMDIs make up approximately 85% of the total pMDI CFP, so switching to inhalers mentioned in this article that have a lower CFP, and ensuring proper medication disposal, will contribute to mitigating the environmental impact of inhalers. In addition, pharmacists should ensure proper inhaler techniques through education and training and question the diagnosis of COPD and asthma when clinically appropriate. Utilizing this information during practice and consistently considering the environmental impact of medications will help push for changes in practice, therapeutic guidelines, and organizational policy (e.g. purchasing practices and formulary choice).
Figure 1. Examples of common inhalers and their low carbon alternatives. Switching from one inhaler to another is only suggested when clinically appropriate and through patient shared decision making. All data presented below is adapted to Canadian equivalents from information provided in the NHS Devon Formulary Guide.19
Image designed by Layne Liberty using free access to canva.com
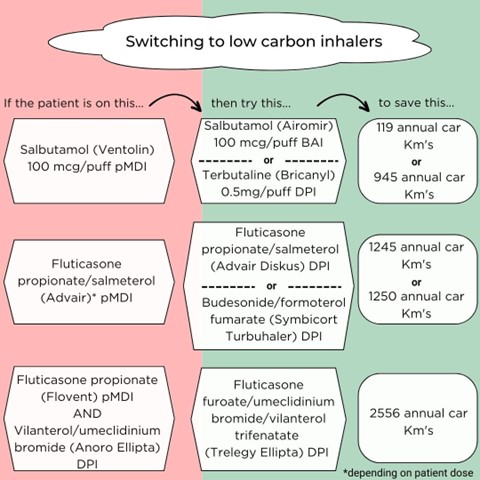
Figure 2. Carbon footprint comparisons of commonly prescribed inhalers.
All data presented below is adapted to Canadian equivalents from information provided in the NHS Devon Formulary Guide19 and PrescQUIPP21
Image designed by Layne Liberty using free access to canva.com
References
- Public Health Agency of Canada. Report from the Canadian chronic disease surveillance system: asthma and chronic obstructive pulmonary disease (COPD) in Canada [Internet]. Ottawa: Government of Canada Publications; 2018. 61 p. Available from: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/asthma-chronic-obstructive-pulmonary-disease-canada-2018/pub-eng.pdf
- Ehteshami-Afshar S, FitzGerald JM, Doyle-Waters MM, Sadatsafavi M. The global economic burden of asthma and chronic obstructive pulmonary disease. The International Journal of Tuberculosis and Lung Disease. 2016;20(1):11-23. Available from: https://doi.org/10.5588/ijtld.15.0472
- Hurst JR, Siddiqui MK, Singh B, Varghese P, Holmgren U, de Nigris E. A systematic literature review of the humanistic burden of COPD. International Journal of Chronic Obstructive Pulmonary Disease. 2021;16:1303-14. Available from: https://doi.org/10.2147/copd.s296696
- Starup-Hansen J, Dunne H, Sadler J, Jones A, Okorie M. Climate change in healthcare: exploring the potential role of inhaler prescribing. Pharmacology Research & Perspectives [Internet]. 2020;8(6). Available from: https://doi.org/10.1002/prp2.675
- Eckelman MJ, Sherman JD, MacNeill AJ. Life cycle environmental emissions and health damages from the Canadian healthcare system: an economic-environmental-epidemiological analysis. PLOS Medicine. 2018;15(7):e1002623. Available from: https://doi.org/10.1371/journal.pmed.1002623
- D'Amato G, Cecchi L, D'Amato M, Annesi-Maesano I. Climate change and respiratory diseases. European Respiratory Review. 2014;23(132):161-9. Available from: https://doi.org/10.1183/09059180.00001714
- Jiang XQ, Mei XD, Feng D. Air pollution and chronic airway diseases: what should people know and do? J Thorac Dis. 2016;8(1):E31-40. doi: 10.3978/j.issn.2072-1439.2015.11.50
- Keeley D, Scullion JE, Usmani OS. Minimizing the environmental impact of inhaled therapies: problems with policy on low carbon inhalers. European Respiratory Journal. 2020;55(2):2000048. Available from: https://doi.org/10.1183/13993003.00048-2020
- CASCADES Canada. Environmentally sustainable opportunities for health systems: Primer Series Inhalers. [Internet]. 2020 [updated 2021 Oct; cited 2023 Feb 22]. Available from: https://view.publitas.com/5231e51e-4654-42c2-accd-b722e21f3093/environmentally-sustainable-opportunities-for-health-systems-primer-series-inhalers/page/12-13
- Woodcock A, Beeh KM, Sagara H, Aumônier S, Addo-Yobo E, Khan J, Vestbo J, Tope H. The environmental impact of inhaled therapy: making informed treatment choices. European Respiratory Journal [Internet]. 2022:60 (1) 2102106. Available from: https://doi.org/10.1183/13993003.02106-2021
- Lindh A, Theander K, Arne M, Lisspers K, Lundh L, Sandelowsky H, Ställberg B, Westerdahl E, Zakrisson A. Errors in inhaler use related to devices and to inhalation technique among patients with chronic obstructive pulmonary disease in primary health care. Nursing Open [Internet]. 2019;6(4):1519-27. Available from: https://doi.org/10.1002/nop2.357
- AL-Jahdali, H, Ahmed, A, AL-Harbi, A, Khan M, Baharoon S, Salih S, Halwani R et al. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Asth Clin Immun 2013:9(8) Available from: https://doi.org/10.1186/1710-1492-9-8
- Environment and Climate Change Canada. Government of Canada [Internet]. Canada’s enhanced nationally determined contribution; 2021. Available from: https://www.canada.ca/en/environment-climate-change/news/2021/04/canadas-enhanced-nationally-determined-contribution.html
- Bridgeman MB, Wilken LA. Essential Role of Pharmacists in Asthma Care and Management. Journal of Pharmacy Practice. 2021;34(1):149-162. doi:10.1177/0897190020927274
- Hudd TR. Emerging role of pharmacists in managing patients with chronic obstructive pulmonary disease. American Journal of Health-System Pharmacy. 2020;77(19):1625-30. Available from: https://doi.org/10.1093/ajhp/zxaa216
- Jia X, Zhou S, Luo D, Zhao X, Zhou Y, Cui Y. Effect of pharmacist‐led interventions on medication adherence and inhalation technique in adult patients with asthma or COPD: a systematic review and meta‐analysis. Journal of Clinical Pharmacy and Therapeutics [Internet]. 2020 Feb 27 [cited 2023 Feb 23];45(5):904-17. Available from: https://doi.org/10.1111/jcpt.13126
- Lin G, Zheng J, Tang PK, Zheng Y, Hu H, Ung COL. Effectiveness of Hospital Pharmacist Interventions for COPD Patients: A Systematic Literature Review and Logic Model. Int J Chron Obstruct Pulmon Dis. 2022;17:2757-2788.
- Rennard SI, Farmer SG. Exacerbations and progression of disease in asthma and chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2004;1(2):88-92. doi: 10.1513/pats.2306026
- North and East Devon Formulary and Referral. Northeast Devon Formulary Guidance NHS [Internet]. The environmental impact of inhalers. Available from: https://northeast.devonformularyguidance.nhs.uk/formulary/chapters/3.-respiratory/the-environmental-impact-of-inhalers#:~:text=Carbon%20footprint,can%20contribute%20to%20global%20warming.
- Fulford B, Mezzi K, Aumônier S, Finkbeiner M. Carbon footprints and life cycle assessments of inhalers: a review of published evidence. Sustainability. 2022;14(12):7106. Available from: https://doi.org/10.3390/su14127106
- PrescQIPP; Homan K. Inhaler carbon footprint 2.2 [Internet]. [place unknown: publisher unknown]; 2021;24 p. Available from: https://www.prescqipp.info/umbraco/surface/authorisedmediasurface/index?url=/media/5719/295-inhaler-carbon-footprint-22.pdf
- Hänsel M, Bambach T, Wachtel H. Reduced Environmental Impact of the Reusable Respimat® Soft Mist™ Inhaler Compared with Pressurised Metered-Dose Inhalers. Adv Ther. 2019 Sep;36(9):2487-2492. doi: 10.1007/s12325-019-01028-y
- Health Product Stewardship Association. Health Products Stewardship Association [Internet]. Returning Medications - Health Products Stewardship Association. Available from: https://healthsteward.ca/consumers/returning-medications/.
- Nguyen TS, Nguyen TLH, Pham TTV, Hua S, Ngo QC, Li SC. Pharmacists' training to improve inhaler technique of patients with COPD in Vietnam. Int J Chron Obstruct Pulmon Dis. 2018;13:1863-1872
- Katsurada, M., Nagano, T., Nakajima, T., Yasuda, Y., Miwa, N., Sekiya, R., Kobayashi, K., Hojo, D., & Nishimura, Y. Retrospective analysis of the effect of inhaler education on improvements in inhaler usage. Respiratory investigation. 2021; 59(3): 312-319 .
- Capstick TG, Burnley M, Higgins H. P234 Improving in inhaler technique: a community pharmacy service.
- Batterink J, Dahri K, Aulakh A, Rempel C. Evaluation of the use of inhaled medications by hospital inpatients with chronic obstructive pulmonary disease. Can J Hosp Pharm. 2012 Mar;65(2):111-8. doi: 10.4212/cjhp.v65i2.1118
- Gerald L, Dhand R. Patient education: Inhaler techniques in adults (Beyond the Basics). In: Basow, DS editor. UpToDate. Waltham, MA: UpToDate; 2021.
- NHS Greater Glasgow and Clyde Area Drug and Therapeutics Committee. GGC Medicines: Home [Internet]. GGC Medicines: sustainability: reducing the environmental impact of inhalers; 2021. Available from: https://ggcmedicines.org.uk/blog/medicines-update/sustainability-reducing-the-environmental-impact-of-inhalers/.
- Canadian Thoracic Society. Choosing Wisely Canada [Internet]. Respiratory Medicine- Seven Tests and Treatments to Question. Available from: https://choosingwiselycanada.org/recommendation/respiratory-medicine/.
- Reddel HK, Bacharier LB, Bateman ED, Brightling C, Brusselle G, Buhl R, et al. Global Initiative for Asthma (GINA) Strategy 2021 - Executive summary and rationale for key changes. Eur Respir J 2021; in press (https://doi.org/10.1183/13993003.02730-2021)
- Aaron SD, Boulet LP, Reddel HK, Gershon AS. Underdiagnosis and Overdiagnosis of Asthma. Am J Respir Crit Care Med. 2018 Oct 15;198(8):1012-1020. doi: 10.1164/rccm.201804-0682Cl
- Walters JA, Walters EH, Nelson M, Robinson A, Scott J, Turner P, Wood-Baker R. Factors associated with misdiagnosis of COPD in primary care. Prim Care Respir J. 2011;20(4):396-402. doi: 10.4104/pcrj.2011.00039
- Zwar NA, Marks GB, Hermiz O, Middleton S, Comino EJ, Hasan I, Vagholkar S, Wilson SF. Predictors of accuracy of diagnosis of chronic obstructive pulmonary disease in general practice. Med J Aust. 2011;195(4):168-71. doi: 10.5694/j.1326-5377.2011.tb03271.x.
- Starren ES, Roberts NJ, Tahir M, O'Byrne L, Haffenden R, Patel IS, Partridge MR. A centralised respiratory diagnostic service for primary care: a 4-year audit. Prim Care Respir J. 2012;21(2):180-6. doi: 10.4104/pcrj.2012.00013.
- Gershon AS, Thiruchelvam D, Chapman KR, Aaron SD, Stanbrook MB, Bourbeau J, Tan W, To T. Health services burden of undiagnosed and overdiagnosed COPD. Chest. 2018;153(6):1336-46. Available from: https://doi.org/10.1016/j.chest.2018.01.038
- Gershon AS, Hwee J, Croxford R, Aaron SD, To T. Patient and physician factors associated with pulmonary function testing for COPD. Chest. 2014;145(2):272-81. Available from: https://doi.org/10.1378/chest.13-0790